
Facial Procedures
Before & After Gallery
The images below document individual patients who have undergone facial surgical procedures: facelift, neck lift, facial fat grafting surgery, eyelid surgery, lip lift. Combined procedures are common; a single set of images may reflect more than one treatment performed during the same operation. Surgical outcomes vary between individuals based on anatomy, skin quality, healing, and other factors. These images are provided for medical information purposes only and do not represent a guarantee, promise, or prediction of outcome for any other patient.
Facelift, Neck Lift and Facial Fat Grafting Surgery


















Eyelid Surgery







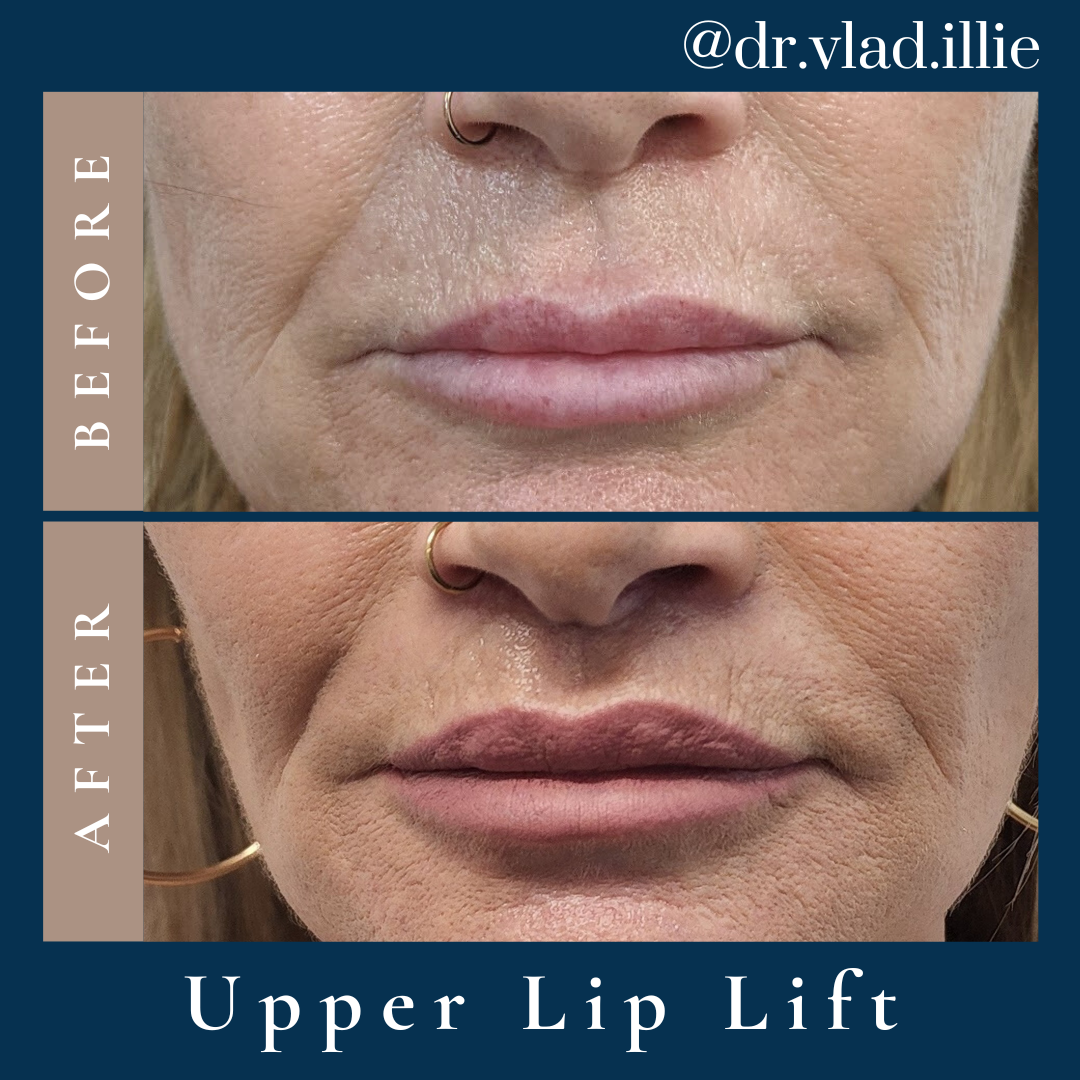
Lip Lift Surgery



Specialist Standards and Safety Protocols for Facial Plastic Surgery
Dr Vlad ILLIE practises in accordance with the professional standards required of a specialist plastic and reconstructive surgeon registered with the Medical Board of Australia. The information below is provided to support informed decision-making.

Qualifications
Dr ILLIE is a specialist plastic and reconstructive surgeon, and he completed the accredited training pathway in Sydney through the Royal Australasian College of Surgeons (RACS). He is a Fellow of:
- FRACS Royal Australasian College of Surgeons
- ASPS Australian Society of Plastic Surgeons
- ASAPS Australian Society of Aesthetic Plastic Surgeons
Dr ILLIE has undertaken post-fellowship training in aesthetic and reconstructive facial and breast surgery, as well as microsurgery in Oxford (UK) and Stuttgart (Germany).
APHRA Registration
Dr ILLIE is registered as a specialist plastic surgeon with the Australian Health Practitioner Regulation Agency (AHPRA), under the Medical Board of Australia.
Registration number:
MED0000966953
Specialist registration with AHPRA means Dr ILLIE has completed an approved specialist training programme and is qualified to hold himself out as a specialist plastic surgeon.
Assessment and Consultation Process
Every patient considering a surgical procedure undergoes two comprehensive clinical consultations with Dr ILLIE prior to any decision being made. This consultation is designed to:
- Review the patient’s medical history, current health status, and medications
- Assess anatomical considerations relevant to the procedure under discussion
- Discuss the patient’s goals and whether they are clinically realistic and appropriate
- Identify any factors that may influence suitability, risk, or likely outcome
- Provide detailed information about the procedure, anaesthesia, recovery, and potential complications
- Allow adequate time for questions from the patient
A wellbeing and psychological assessment is also done before the decision to proceed with surgery.
Mental Health Support
In addition to physical assessment, Dr ILLIE’s consultation process includes consideration of each patient’s psychological readiness for elective surgical intervention. This forms a routine component of the clinical assessment for all aesthetic procedures and also includes the mandatory screening regulated by AHPRA.
Where there are concerns about a patient’s psychological state, motivation, or expectations, Dr Illie may recommend a period of further reflection, provide further support and clarity to the patient, decline to proceed or refer the patient to an appropriate mental health professional before any surgical decision is made. This process is undertaken in the patient’s best interests and does not reflect the patient’s suitability as a person.
Informed Consent
Informed consent is a legal and ethical requirement for all surgical procedures. Dr ILLIE’S consent process involves providing each patient with:
- A clear explanation of what the procedure involves
- The known risks, potential complications, and likelihood of each
- Realistic information about expected recovery and healing timelines
- A discussion of alternative options, including non-surgical approaches where relevant
- Time to review written material before signing any consent documentation
Consent is obtained during consultation, prior to surgery — not on the day of the procedure. Patients are encouraged to bring a support person and to raise any questions that arise after the initial consultation.
Individualised Medical Advice
No information on this website — including before-and-after photographs — constitutes medical advice. The images in this gallery document individual cases and are provided as a general reference only. They do not represent typical, average, or expected outcomes for any prospective patient.
Decisions regarding surgical intervention should only be made following a face-to-face clinical consultation in which Dr ILLIE can review your specific circumstances. The advice provided in your consultation is personal to you and cannot be inferred from information published online or from other patients’ experiences.
All surgical procedures carry inherent risks. A full discussion of risks and complications is available at Risks & Complications.
Frequently Asked Questions
What is Dr ILLIE'S approach to facelift surgery, and how does he plan the procedure?
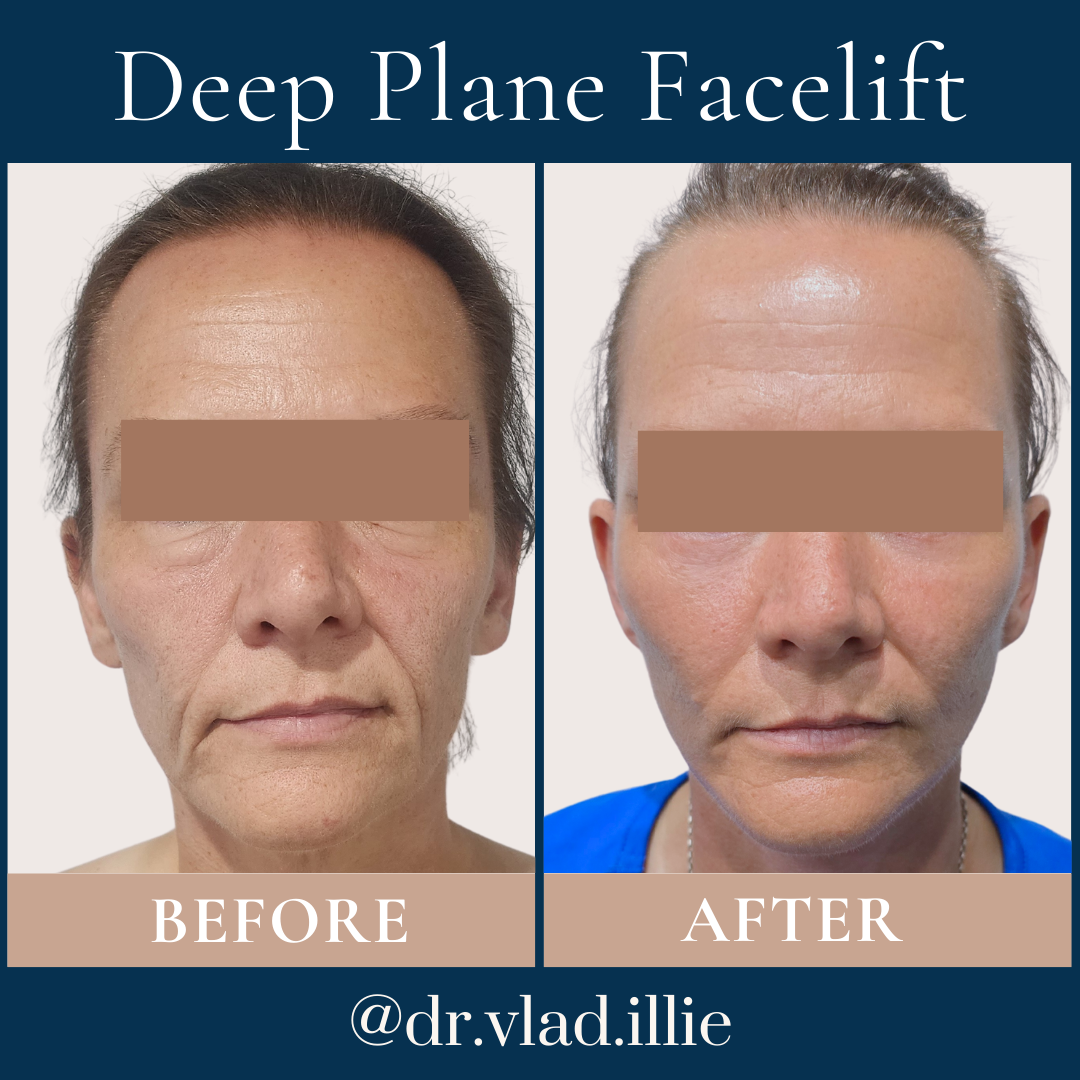
Dr Vlad ILLIE approaches facelift surgery with what he describes as a commitment to personalised planning and safe, long-lasting natural results. He completed specialist training in Sydney and undertook additional post-fellowship training in facial reconstruction and cosmetic surgery in Oxford (UK) and Stuttgart (Germany), which has informed his understanding of the full spectrum of facial anatomy — from the superficial skin layers through to the deep structural planes.
In planning a facelift, Dr ILLIE begins with a thorough anatomical assessment of each patient. He examines the degree and distribution of skin laxity, the condition of the SMAS (superficial musculoaponeurotic system — the deeper structural layer beneath the skin), the extent of jowling, the position of the midface soft tissue, and the condition of the neck. Not every patient requires the same technique: some patients are best served by a lower facelift; others by a deep plane approach that addresses the deeper structural layer; others by a more limited procedure such as a mini facelift. Dr ILLIE selects the technique based on the patient’s anatomy and goals, not a one-size-fits-all approach.
During the consultation, Dr ILLIE takes time to explain what the procedure involves in practical terms, what recovery looks like, what is realistic to expect given the patient’s specific anatomy, and where the incisions will be placed and why. He emphasises that the goal of facelift surgery is not an artificially altered appearance but a result that looks natural and continues to feel appropriate over time. Patients are encouraged to ask questions and, where needed, to attend more than one consultation before making a decision.
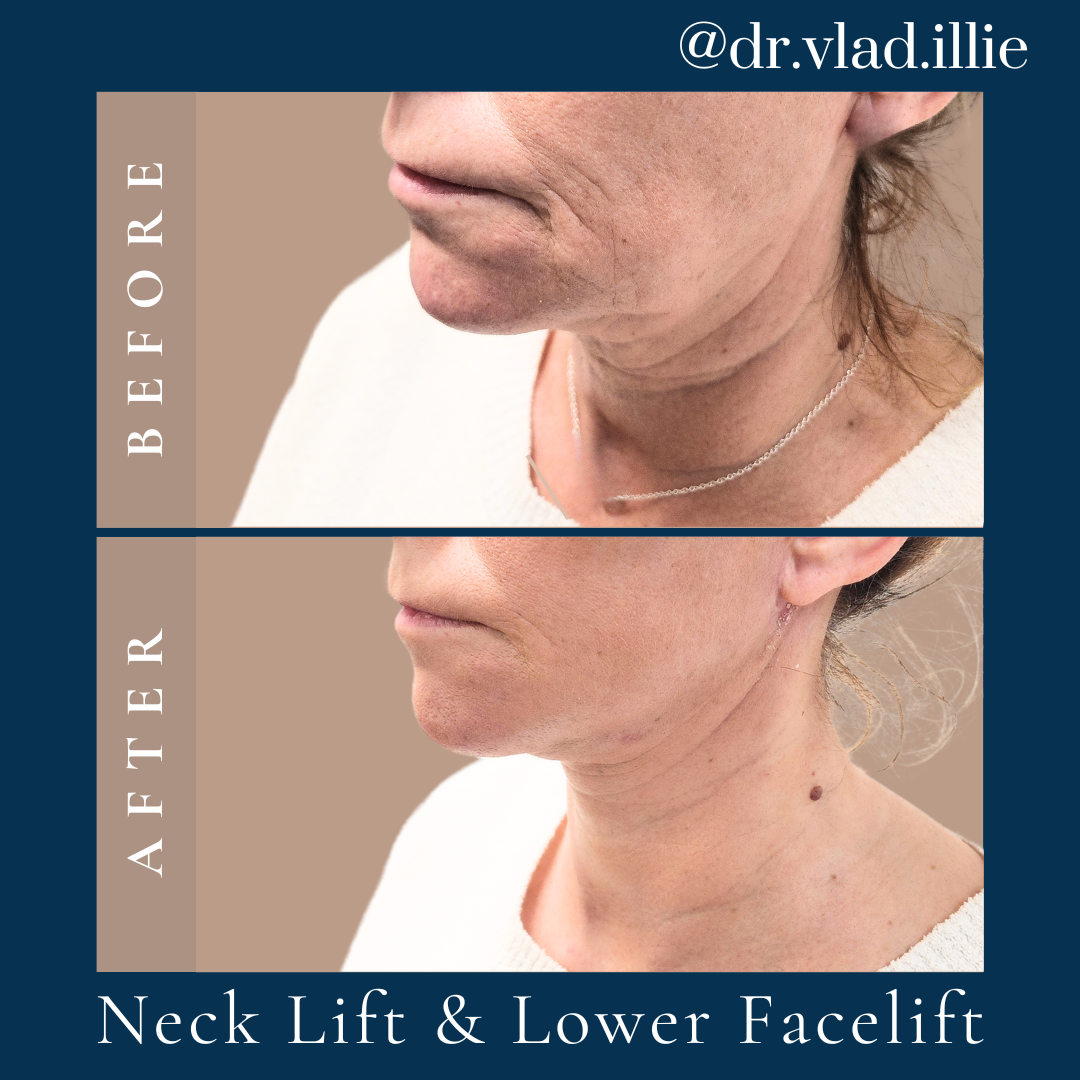
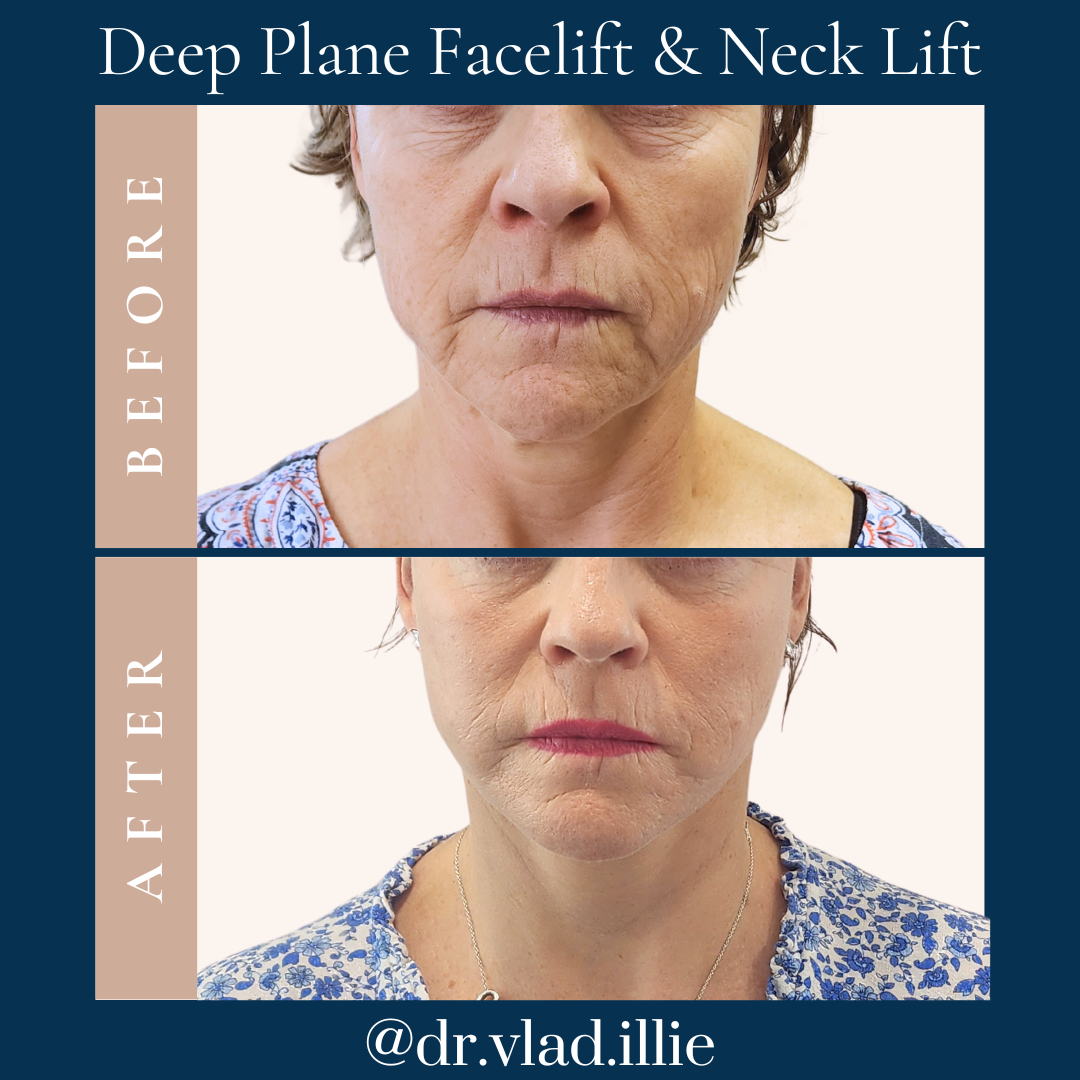
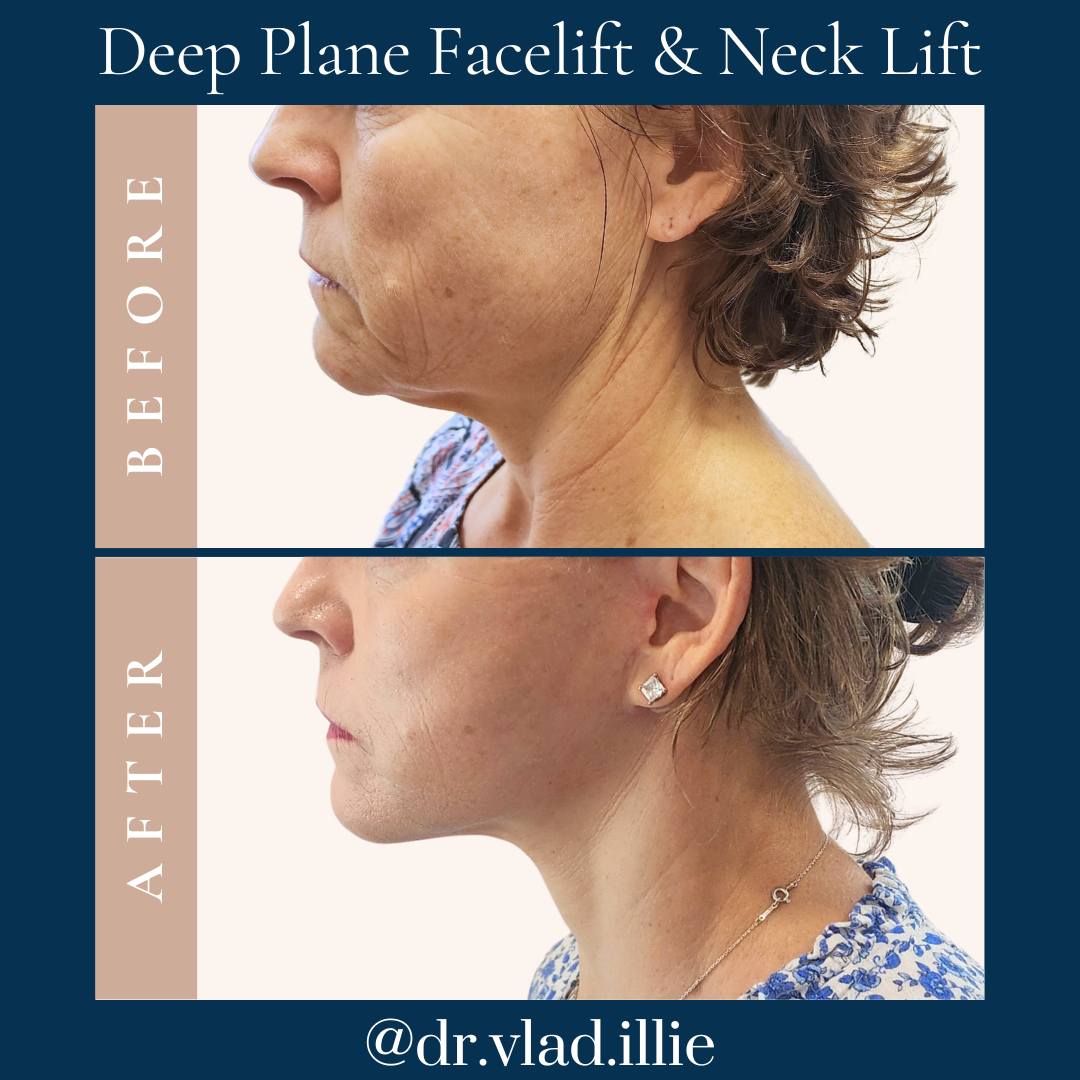
Why does Dr ILLIE often combine facelift with neck lift surgery?
The face and neck are anatomically continuous, and the ageing changes that affect the lower face — jowling, descent of the midface soft tissues, loss of jawline definition — are frequently accompanied by concurrent changes in the neck, including skin laxity, platysmal banding, and submental fullness (double chin). For many patients, addressing the lower face without addressing the neck at the same time would leave a visible inconsistency between the two areas. Dr ILLIE assesses each patient’s neck independently during the consultation and makes a clinical recommendation based on his observations.
When a facelift and neck lift are performed together, they are undertaken through incisions planned to work in a coordinated way — the incision placement is designed to allow Dr ILLIE to address both areas without creating additional visible scarring. The neck component may involve addressing the platysma muscle to improve neck contour and sharpen the cervicomental angle, as well as removing or redistributing excess skin and submental fat, where present.
Dr ILLIE is clear that combining procedures is a clinical decision, not a commercial one. Patients for whom a neck component is not indicated are not recommended to have one, and patients for whom a staged approach is more appropriate are advised accordingly. His goal is a coherent, natural-looking result for the overall face and neck — not the completion of a procedure list.
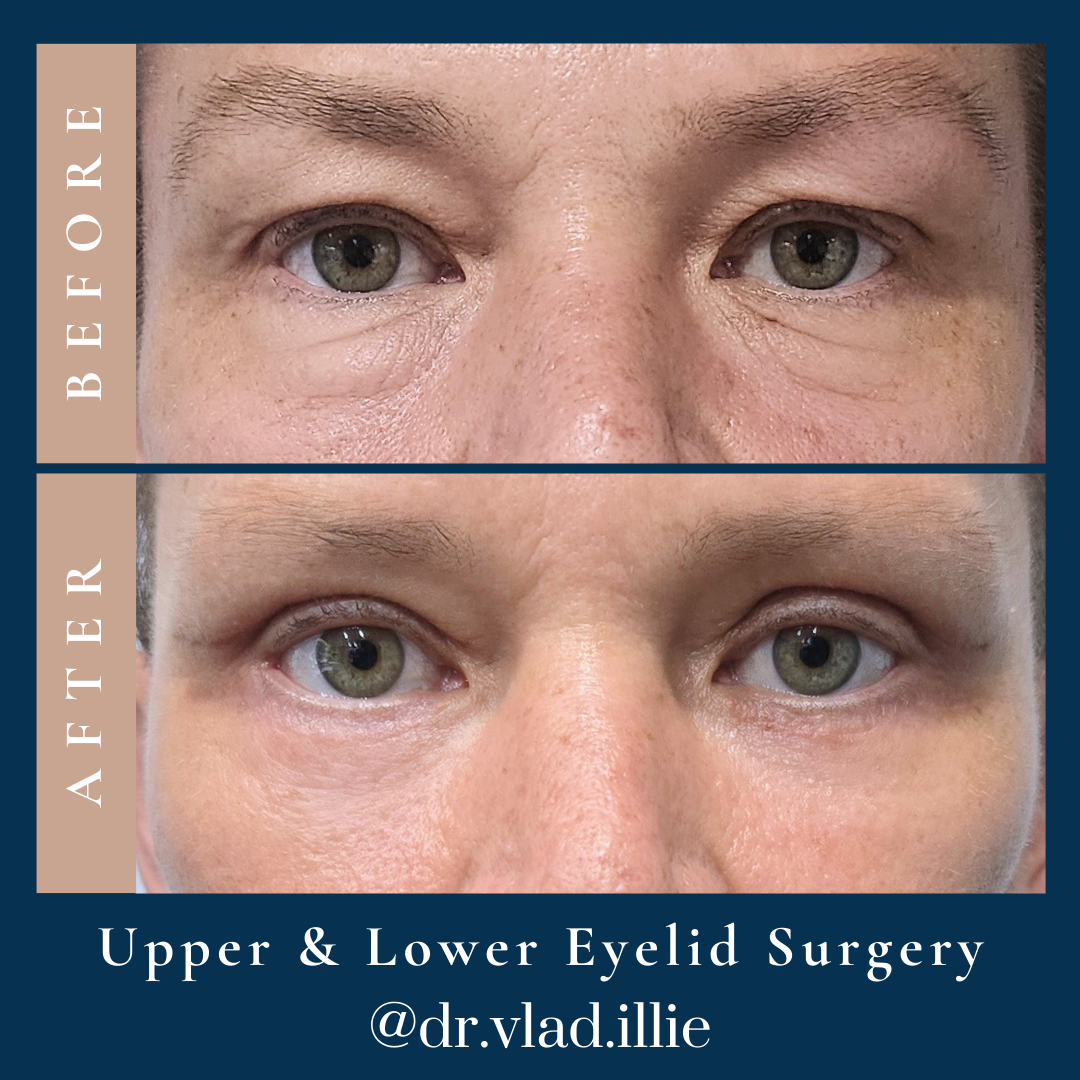
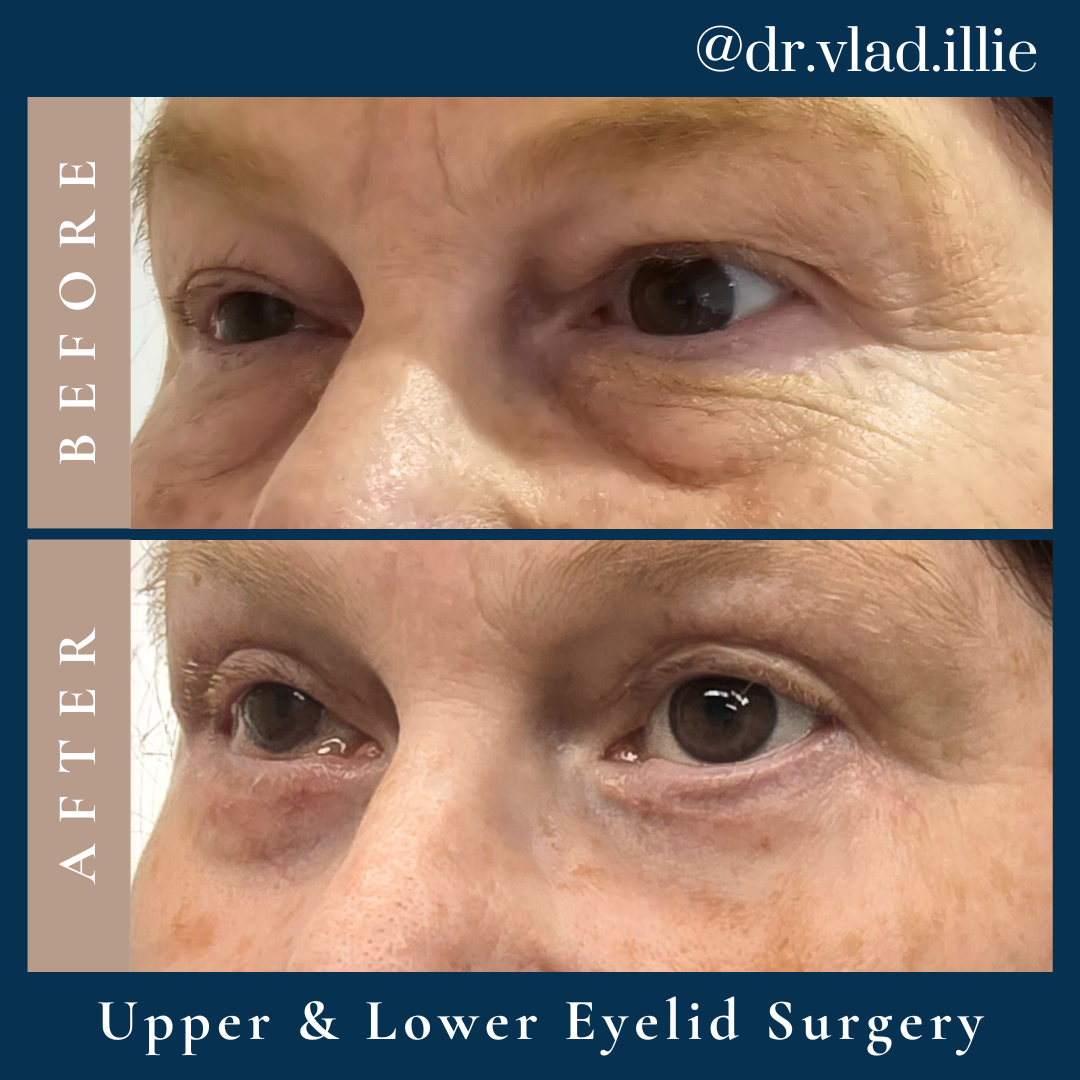
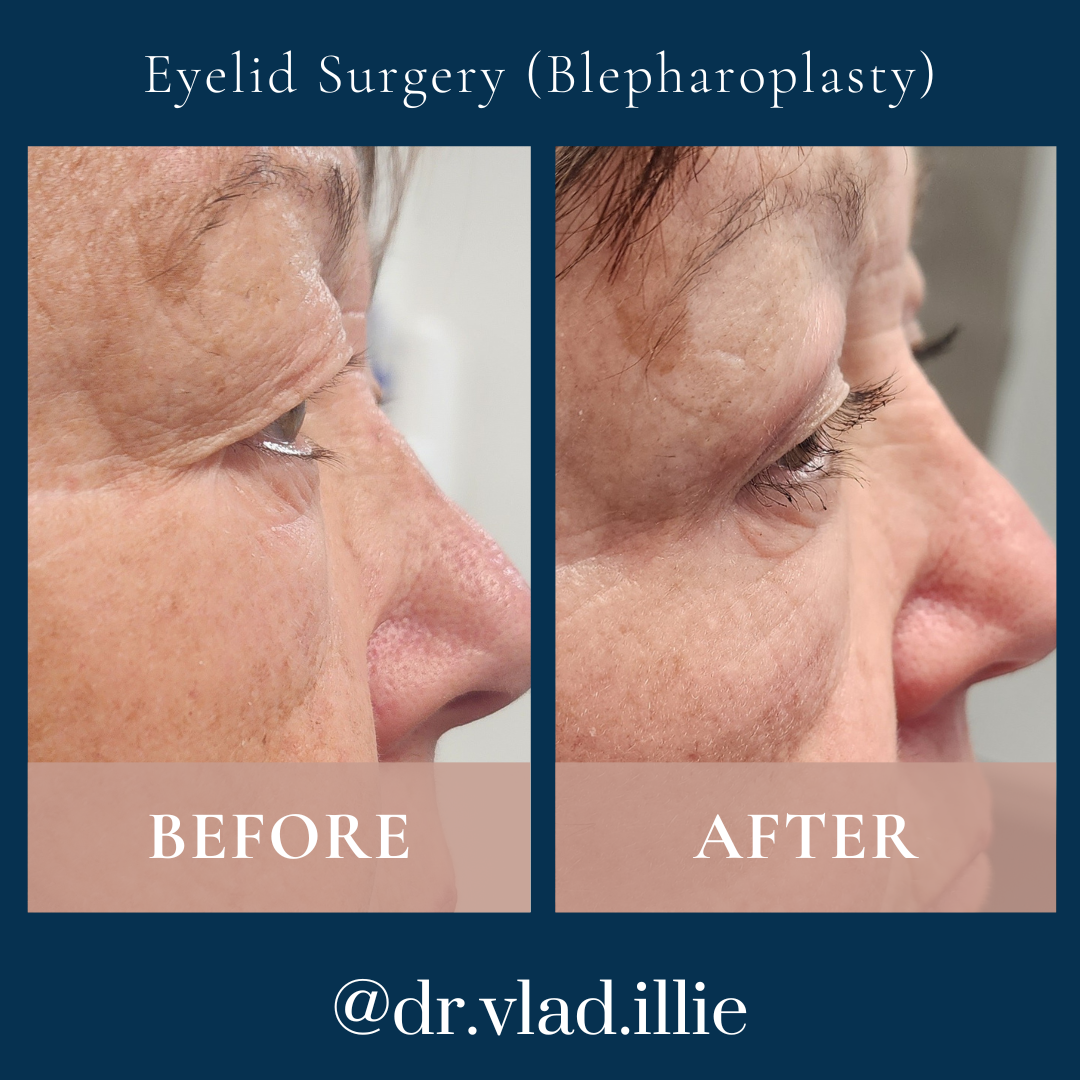
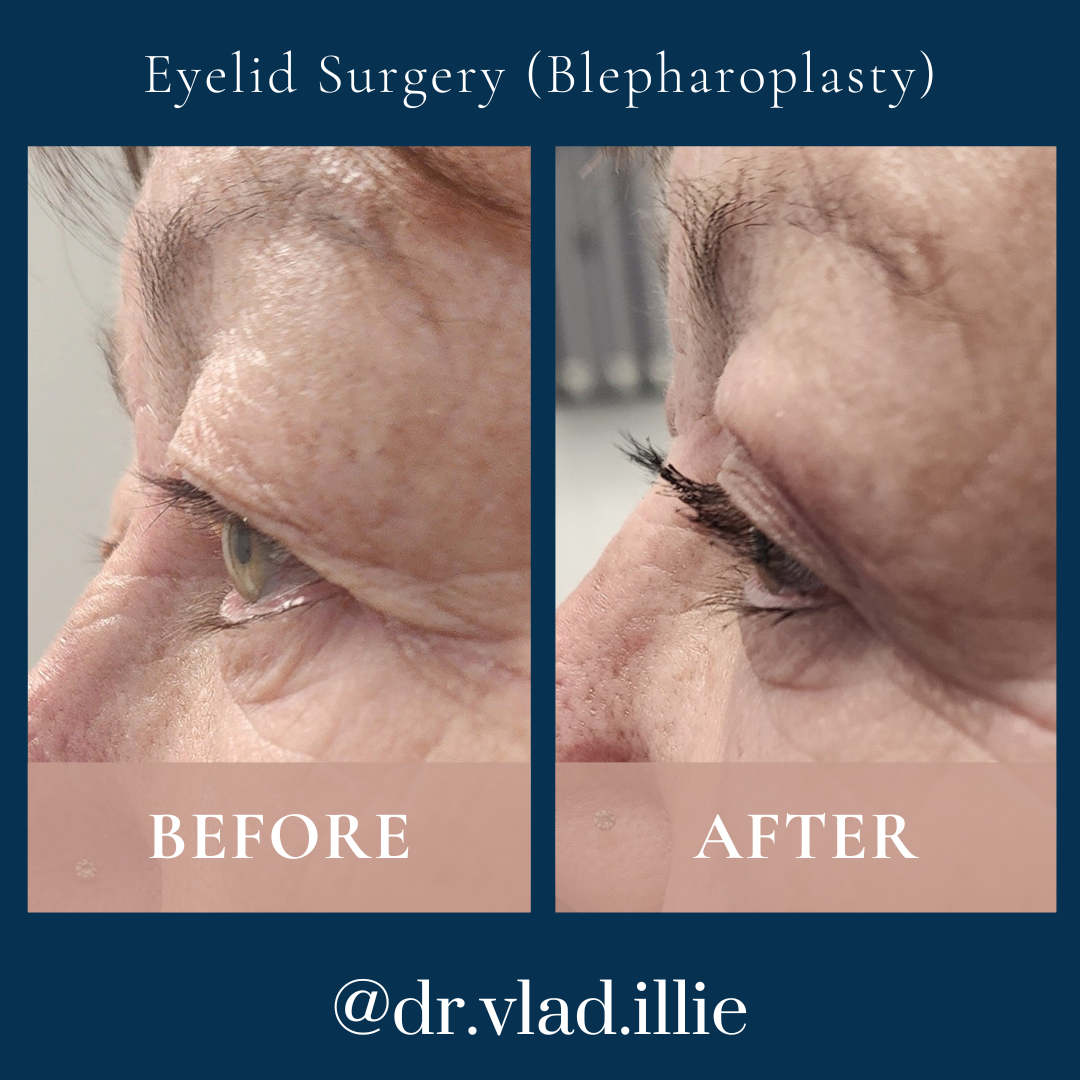
How does Dr ILLIE approach eyelid surgery (blepharoplasty), and what does assessment involve?
Blepharoplasty — eyelid surgery — is one of the most anatomically precise procedures in facial surgery. The periorbital area involves multiple tissue layers in close proximity, and achieving a result that looks natural, well-rested, and symmetrical requires careful preoperative planning and meticulous surgical technique. Dr ILLIE’S approach to eyelid surgery begins with a detailed assessment of the patient’s periorbital anatomy, including the degree of upper eyelid skin redundancy, the position of the brow, the presence and degree of lower eyelid fat prolapse, the quality of the lower eyelid skin, and the structural support of the lower eyelid margin.
A critical part of Dr ILLIE’S assessment is determining whether upper eyelid heaviness is being driven by excess eyelid skin itself, by descent of the brow (ptosis of the brow), or by both. These two situations require different surgical approaches, and incorrectly attributing one to the other can lead to a suboptimal result. For patients in whom brow descent is a meaningful contributor, Dr ILLIE may discuss brow lift surgery as part of a broader plan or advise on the limitations of eyelid surgery alone in addressing the presentation.
For lower eyelid blepharoplasty, Dr ILLIE assesses the structural integrity of the lower eyelid — a relevant factor in planning the technique — and the patient’s tear film and dry eye history, as lower eyelid surgery can affect tear drainage and ocular comfort. The assessment is thorough because the periorbital area is one where patient satisfaction and clinical precision must be closely aligned.
Dr ILLIE has performed eyelid surgery as a standalone procedure and as part of combined facial rejuvenation plans. He discusses all of this in detail during the consultation, so that patients understand exactly what will be done, why, and what to expect during recovery.
What is facial fat grafting, and why does Dr ILLIE include it in some facial surgery plans?
Facial fat grafting — also called facial fat transfer — involves harvesting small amounts of the patient’s own fat from a donor site (typically the abdomen or inner thigh), processing it, and transferring it to specific areas of the face to restore volume. Dr ILLIE uses this technique because facial ageing involves not only the descent and loosening of soft tissues addressed by a facelift, but also a loss of volume in key facial regions — the temples, the cheeks, the area beneath the eyes, and around the lips and mouth. For some patients, tissue repositioning alone does not fully address the three-dimensional changes of facial ageing; volume restoration through fat grafting can complement the structural work of the facelift.
Dr ILLIE has training and experience in complex surgical techniques that inform his fine-level anatomical tissue handling, which carries over into the precision with which fat grafting is performed. The fat is transferred in small, carefully placed deposits to maximise the likelihood of graft survival and achieve a smooth, natural contour rather than an uneven or lumpy result.
He is also transparent with patients about the biology of fat grafting: a proportion of transferred fat is reabsorbed by the body over the weeks following surgery, and the final volume after graft take is established over several months. The degree of retention varies between individuals and cannot be precisely predicted in advance. When fat grafting is included in a surgical plan, Dr ILLIE discusses it specifically — the donor site, the recovery implications, and the likely contribution to the overall result.
What does Dr ILLIE'S approach to lip lift surgery involve, and who is it suitable for?
The upper lip lift — also called a subnasal lip lift — is a surgical procedure that shortens the distance between the base of the nose and the upper lip border (the philtrum), which tends to lengthen with age and can give the lip a flattened, elongated appearance. Dr ILLIE assesses suitability for this procedure by measuring the philtrum height and evaluating the proportions of the lower face, the degree of lip show at rest, and the patient’s overall facial balance. It is a procedure where subtle anatomical precision matters considerably: the incision is placed in the base crease of the nose, and the amount of skin removed is planned carefully to achieve a natural-looking result without distorting the nasal base or creating an overly pronounced appearance.
Dr ILLIE discusses with each patient what the procedure can and cannot achieve. A lip lift addresses the vertical dimension of the philtrum and can increase the appearance of the upper lip border at rest, but it does not add volume in the way that injectable fillers do, and it is not appropriate for all patients presenting with concerns about the lips. Where the philtrum length is not the primary issue, Dr ILLIE will explain this and discuss what other options may be more relevant to the patient’s anatomy.
The procedure is frequently performed under local anaesthesia with sedation as a day procedure, and recovery is relatively straightforward compared with more extensive facial surgery. Dr ILLIE takes care to discuss scar management after lip lift surgery, as the scar position — while well-concealed — is in a visible area and requires appropriate post-operative care during the healing period.
Why do results vary so much between patients, even for the same facial procedure?
Facial surgery acts on tissue that is profoundly individual. Two patients can present with what looks like a similar concern — jowling, for example, or upper eyelid heaviness — and yet have fundamentally different underlying anatomies, skin qualities, and healing biologies. Dr ILLIE addresses this directly with every patient: the result that appears in a photograph is a product of the interaction between the surgical technique, the patient’s specific anatomy, and the patient’s individual healing response. None of these three factors is the same between any two patients.
Skin quality is one of the most variable factors. Skin that is fine and elastic responds differently to the tension and repositioning involved in a facelift than skin that is thicker, more sun-damaged, or less elastic. The depth and distribution of facial fat, the thickness of the SMAS layer, the degree of bony projection underlying the soft tissue — all of these are individual features of each patient’s face that shape what can be achieved surgically and what the result will look like.
Healing variability adds a further layer. Some patients experience prolonged swelling; in others it resolves quickly. Collagen remodelling — which continues for many months after surgery and contributes to the long-term feel and firmness of the operated tissue — proceeds at different rates in different individuals. These are not things that Dr ILLIE or any surgeon can control; they are part of the biology of each patient. What Dr ILLIE can control is the thoroughness of his planning, the quality of his technique, and the support he provides his patients through the recovery process.
How does Dr ILLIE'S consultation process work for facial surgery?
Dr ILLIE’S consultation process is built around taking time with each patient and making sure that all relevant information is genuinely understood. He meets with every patient personally — the consultation is with Dr ILLIE himself, not a patient coordinator or nurse practitioner — and he conducts a thorough assessment of the patient’s facial anatomy, medical history, and the concerns they have come to discuss.
During the consultation, Dr ILLIE listens carefully to what is bothering the patient and what they hope surgery might address. He then examines the anatomy relevant to those concerns, explains what he observes, and discusses the options available — including the honest limitations of each. He is direct about cases where he believes surgery is not the most appropriate option, or where the patient’s expectations may not align with what a procedure can clinically deliver. He considers this part of his responsibility to the patient.
The consultation includes a discussion of surgical risks and complications specific to the procedure being considered, because Dr ILLIE believes that fully informed consent is not an administrative formality — it is a clinical and ethical requirement that he takes seriously. Patients are given the opportunity to ask questions, and are usually given further information to read before the second consultation. Surgery is never booked during the first appointment.
Dr ILLIE operates at St Vincent’s Private Hospital, Bondi Junction Private Hospital, East Sydney Private Hospital and Gosford Private Hospital. His work spans both aesthetic and reconstructive surgery, and this breadth of practice informs his clinical judgement in ways that benefit his aesthetic patients.
Can I tell from the photos in this gallery what my own result might look like?
No — and this is something Dr ILLIE is direct about with every patient who raises the topic. The photographs in this gallery document individual patients under their specific anatomical, biological, and circumstantial conditions. They are factual records of what happened in those particular cases. They cannot be used to predict or infer what a different patient will experience, because no two patients have identical anatomy, identical skin, or an identical healing biology.
What a gallery can usefully convey is the range and character of Dr ILLIE’s work across different patient types and different procedures. It demonstrates that his surgical approach produces results across a variety of presentations. But the specific visual outcome in any photograph belongs to that patient and that patient alone. The only way to understand what may be possible in your own case is through a direct clinical assessment.
Can I ask Dr ILLIE to see additional cases during my consultation?
Yes. Additional examples of surgical cases may be available for review in a clinical setting, depending on patient consent and the availability of cases relevant to your particular circumstances. Consent for the use of medical photographs is sought separately and voluntarily from each patient, and the cases available at any given time reflect those where consent has been provided.
During your consultation with Dr ILLIE, you are welcome to ask whether cases relevant to your own anatomy, age group, or specific procedure of interest are available to review. Where they are, Dr ILLIE can discuss the clinical context of those cases with you — the presenting anatomy, what was done, and the timeline of the documentation. This can be a useful part of the consultation discussion, though the same principle applies: cases viewed in the clinical setting are examples of individual documented outcomes and cannot be used to predict your own result.
What should I bring to my first consultation with Dr ILLIE about facial surgery?
Dr ILLIE’S consultation is most useful when he has access to relevant health information and when the patient arrives with a clear sense of what they want to discuss. From a health perspective, it is helpful to bring a list of current medications — including prescription medications, over-the-counter items, vitamins, and supplements — as a number of commonly used medications affect bleeding, healing, and anaesthetic risk. Any significant medical history, including prior facial or neck surgery, blood thinning conditions, autoimmune conditions affecting the skin or connective tissue, or a history of keloid or hypertrophic scarring, is relevant to disclose.
From a personal perspective, the most useful preparation is a clear and honest account of the concerns you want to discuss — what is bothering you, for how long, and what prompted you to consider surgery now. Dr ILLIE does not expect patients to arrive with a specific procedure in mind; that is his role to advise on. What he does value is an honest conversation about what matters to the patient and why. The more clearly a patient can articulate their concerns in their own words, the more useful and efficient the consultation will be.
There is no obligation to make any decision at a first consultation with Dr ILLIE. It is an assessment and information-gathering appointment, and patients leave with a clear understanding of what options are available, what would be involved, and what to expect — not a signed surgical form. If further reflection time is needed, this is considered when booking the second consultation.